








Androgenic alopecia (AGA) is a common type of hair loss caused by heredity and hormones, which is characterized by thinning scalp hair. Among the 60 year olds, 45% of men and 35% of women are facing the problem of AGA. FDA approved AGA treatment protocols include oral finasteride and topical minoxidil. At present, due to the lack of effective treatment, PRP has become a new and promising alternative therapy. A large number of growth factors in PRP can promote hair regeneration and platelet α A variety of growth factors secreted by the granules act on the stem cells in the hair follicle bulge area and stimulate the formation of new blood vessels. Although many articles have reported this, there is no standardized protocol for PRP preparation, route of administration and evaluation of clinical results. This article aims to evaluate the effectiveness of PRP in the treatment of AGA and explore various existing treatments.
Action mechanism of PRP:
PRP is activated after being injected into scalp to release a large number of growth factors and promote hair growth. These growth factors can activate fibroblasts, promote collagen synthesis, improve extracellular matrix secretion and regulate the expression of endogenous growth factors. Growth factors (PDGF, TGF- β、 VEGF, EGF, IGF-1) can promote cell proliferation and differentiation, chemotactic stem cells, induce long hair development, and promote hair follicle angiogenesis. Other factors (serotonin, histamine, dopamine, calcium and adenosine) can increase membrane permeability and regulate inflammation.
PRP preparation:
All PRP preparation schemes follow a general rule, and anticoagulants (such as citrate) are added to the collected blood to avoid spontaneous coagulation and platelet activation. Centrifuge to remove red blood cells and concentrate platelets. In addition, many schemes choose exogenous platelet activators (such as thrombin and calcium chloride) to promote the rapid release of growth factors from platelets in a dose dependent manner. Inactivated platelets can also be activated by dermal collagen or autothrombin. Generally, active growth factor is secreted 10 minutes after activation, and 95% of the synthesized growth factor is released within 1 hour, lasting for 1 week.
Treatment plan and concentration:
PRP is usually injected subcutaneously or intradermally. At present, the optimal treatment frequency and interval have not been established. The concentration of PRP is an important factor affecting the clinical effect. Seven articles included put forward that the optimal concentration of PRP is 2~6 times, and excessive concentration will inhibit the angiogenesis. There is still a dispute about whether it contains white blood cells.
The current research results show that PRP can be used in the treatment of AGA. Seven of the nine studies described positive results. The efficacy of PRP was evaluated from multiple perspectives: PTG detection method, hair tension test, hair count and hair density, growth period to rest period ratio, and patient satisfaction survey. Some studies only reported the improvement effect of 3-month follow-up after PRP treatment, but lacked 6-month follow-up results. Some long-term follow-up studies (6 to 12 months) reported a decrease in hair density, but it was still higher than the baseline level. Side effects were reported only as transient pain in the injection area. No adverse reactions were reported.
Recommended treatment:
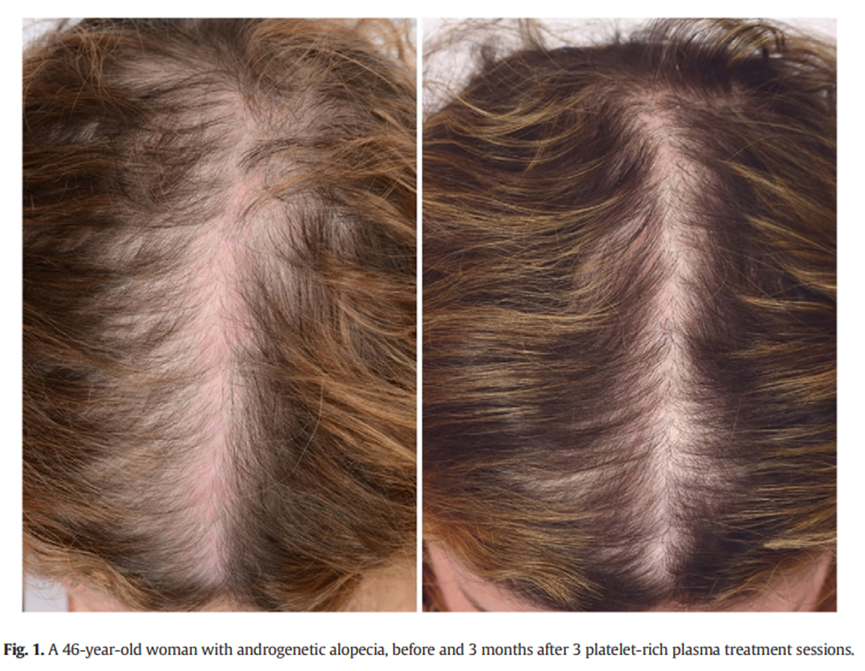
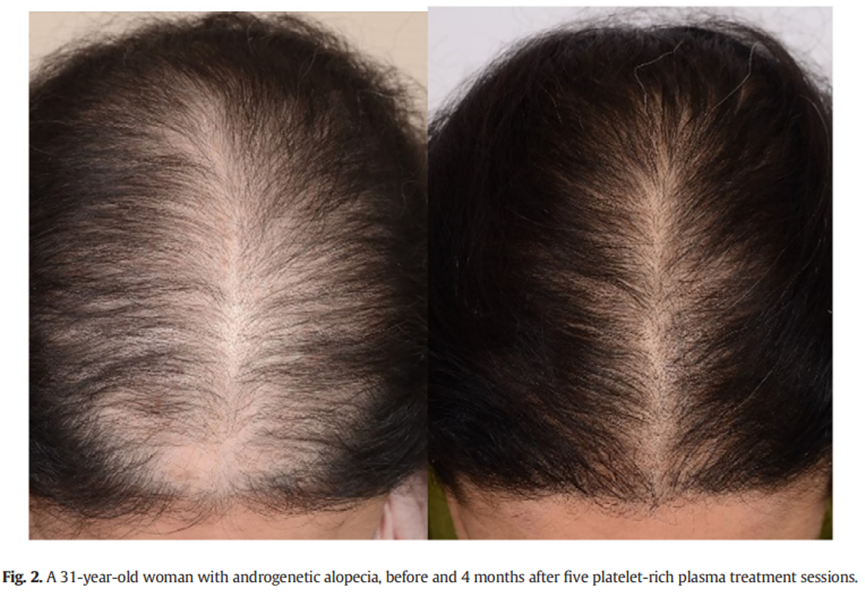
Since PRP does not inhibit the hormone level related to AGA, it is recommended that PRP be used as an adjuvant therapy for AGA. Therefore, patients should be encouraged to maintain topical or oral medication (such as minoxidil, spironolactone and finasteride). Based on this retrospective study, it is recommended to prepare P-PRP (leukopenia) with a concentration 3-6 times that of whole blood. The use of activators (calcium chloride or calcium gluconate) before treatment helps to release growth factors. It is suggested that subcutaneous injection should be carried out from the part with sparse hair, along the hairline and overhead, and the injection sites should be separated. The injection dose is determined by clinical needs. The injection frequency is selected for the first course of treatment (once a month, three times in total, three months), and then once every three months, three times in total (that is, once in June, September and December respectively). Of course, after the first course of treatment, it is also effective to change the interval time to once every six months. In general, male and female patients have achieved positive results in hair regrowth, hair density increase and quality of life improvement after injecting PRP to treat AGA (Picture 1 and Picture 2).
Conclusion:
The review of several research results shows that PRP is promising in the treatment of AGA. At the same time, PRP treatment seems to be safer and less side effects. However, there is still a lack of standardized PRP preparation method, concentration, injection scheme, dosage, etc. Therefore, it is difficult to evaluate the clinical efficacy of PRP. In order to further study the effect of PRP on hair regeneration in AGA, a larger sample size of randomized controlled trial (note the injection frequency, PRP concentration, and achieve long-term follow-up) is required.
(The contents of this article are reprinted, and we do not provide any express or implied guarantee for the accuracy, reliability or completeness of the contents contained in this article, and are not responsible for the opinions of this article, please understand.)
Post time: Dec-08-2022